In labour, shorter doesn't necessarily equate to better OR easier!
Besides the usual interventions that are pushed on labouring mothers by the medical system to rush things along, which are most of the time completely unnecessary and cause more problems and a cascade of further medical interventions, the very real fact is that rushing birth is not helping the mother or the baby (except in the rare cases of true medical emergencies).
I have written (and experienced) about all these supposedly necessary medical interventions that are pushed on mostly unknowing mothers. I will not rehash all the reasons that these interventions are dangerous and unneeded in 99% of labours.
I want to focus on the actual topic of "fast and slow", normal and unnormal, better and worse.
I, like many other mothers out there, have been green with envy when hearing that this friend or that one had a 3 hour labour... "oh you're sooooo lucky!!"
But the truth is that most of the women that I've spoken with who had super fast labours were even more traumatized by their birthing experience than many mothers I know who've laboured for 18 hours. Why? Because the suddenness and going from 0 to 100km/hr so fast did not give them the time they needed- physically, emotionally or energetically- to find their center or that balance point that can flow WITH the labour, instead of being slammed by the tidal waves of contraction on top of contraction.
Faster does NOT equal better.
As for what is perceived to be "normal" in labour, yet again we run into the wall of unrealistic expectations and the medical machine that wants to process all labouring women with a cookie cutter. What is normal for one woman and one birth is not necessarily normal for another woman or even another birth! I have one friend who's first baby was born after 10 hours of labour, 3 hours of stalled labour IN transition, then 4 hours of pushing. Her next child was almost born in the car on the way to the hospital!! Both labours were perfectly "normal" and yet if she had of had midwives, she would of been forced into an unnecessary Cesarean Section with her first child and probably into an elective C/Section with her second because,.... you know, she obviously wasn't capable of birthing naturally. lol
This is the very same in all aspects of pregnancy, labour, birth, and the beautiful babies that are born. When you try to compare and create a paradigm of "normal" or "not normal", instantaneously you are setting an unrealistic president.
I love that the studies are now proving that these cookie cutter labours are not working. Now it's up to all of us to make sure that this information gets out- not just to the public, but to the hospitals and doctors AND midwives as well!
It only by challenging the accepted "norm" that we can CHANGE it.
Study Suggests Misplaced Fears in Longer Childbirths
Launch media viewer
A
new study in the journal Obstetrics and Gynecology suggests that women
in labor may be subject to unnecessary interventions by doctors who
wrongly fear labor has become prolonged.Laura Segall for The New York Times
Epidural anesthesia lengthens the second stage of labor, the one in which women push. But a study published on Wednesday
has found that epidurals are associated with an even longer duration in
the second stage than is generally recognized, suggesting that some
women may be subject to unnecessary interventions by doctors who wrongly
fear labor has become prolonged.
The
finding indicates that “clinicians might need to wait later before
intervening with oxytocin, forceps, vacuum or a cesarean,” said Dr. S.
Katherine Laughon, an investigator at the National Institutes of Health
who was not involved in the study, which was published in Obstetrics and
Gynecology. Still, she added, “clinicians and women need to balance
benefits of vaginal delivery with potential increases in risk for mom
and baby.”
The
new study suggests a normal second stage can take as long as 5.6 hours
for women who get epidurals during their first births, and as long as
3.3 hours for those who do not get epidurals.
For
women who have given birth previously, the group’s guidelines define an
unusually long second stage as two hours with an epidural, one hour
without. The new study found that the second stage for these women can
be as long as 4.25 hours and 1.35 hours, respectively.
“This
paper is very important, and ACOG needs to update its 2003 guidelines,”
said Dr. Robert L. Barbieri, chairman of obstetrics and gynecology at
Brigham and Women’s in Boston, who was not involved in the new study. He
added, “I will change my practice and feel more comfortable going to
five and a half hours with a first birth after an epidural with
reassuring fetal monitoring.”
Researchers at the University of California, San Francisco,
analyzed the records of 42,268 women who delivered vaginally without
problems between 1976 and 2008. Roughly half had epidurals.
The
investigators compared the average length of the second stage of labor
among women who had epidurals with that among women who did not. They
also compared the upper limits of duration for both groups.
Thirty-one
percent of first births and 19 percent of subsequent labors would have
been classified as abnormally long by the current ACOG definition, the
researchers found.
“It’s
time to re-examine what normal and abnormal is, and revise our
guidelines based on modern obstetric population,” said Dr. Yvonne W.
Cheng, the lead author of the study and an associate professor of
obstetrics and gynecology at the University of California, San
Francisco.
The
research is part of a growing body of evidence suggesting that a normal
second stage of labor is now longer than it was decades ago. In 2010, a study of more than 62,000 women found it was as long as 3.6 hours for first-time mothers after an epidural, and 2.8 hours for women who did not get one.
But this latest study is the first to suggest such an extended second stage may be ordinary.
“One
of the messages of this study is, sit on your hands a little longer,
don’t rush into an instrumental vaginal delivery or a cesarean, because
really everything could be fine,” said Dr. Barbara Leighton, a professor
of anesthesiology at Washington University in St. Louis School of
Medicine, who has researched the effects of epidurals on labor.
But
while Dr. Leighton supports revising ACOG recommendations, she believes
that the current study did not prove that longer labor is caused by
epidural anesthesia. Women who request anesthesia may be predisposed to
longer labor for other reasons, she said.
Dr.
Jeffrey Ecker, the chairman of the committee on obstetrics practice for
ACOG, said today’s clinicians are “increasingly recognizing there can
be healthy outcomes and vaginal deliveries of healthy babies when the
second stage extends beyond how it’s traditionally been defined.”
He
added, “Often what’s best and most appropriate — and most difficult —
during labor is patience.” He would not say whether a revision of
guidelines is in the works.
Patience
during labor is not risk-free. The new study found that babies are more
likely to have birth trauma, such as a bruise on the head or a clavicle
fracture,
after longer second-stage labor. But these infants did not have lower
scores on tests designed to measure physical health in newborns, nor did
they experience more admissions to intensive care.
The
risks of significant perineal lacerations and postpartum hemorrhage
were higher in women who experienced prolonged second-stage labor, both
by ACOG’s definition and by the upper limits of the study’s definition
of normal.
While
Dr. Laughon applauded the large number of participants in the study,
she cautioned that “they are saying we should wait longer, but we still
don’t know if that’s safe.”
A
lot has changed since the 1950s, when labor progression norms were
established. Back then, more babies were delivered by forceps and
continuous fetal monitoring was not used.
“We
are doing less interventions to facilitate a shorter second stage, and
we’re letting the power of the uterus and a mother’s pushing determine
the length of the second stage,” Dr. Barbieri said.
One of the most coherant and well defined and articulate articles that I've read in a long long time. Every single point that is made here is vitally important, not only during pregnancy and birth of your child, but through out life in general.
Understanding good and bad bacteria, "anti" bacterials, "anti" biotics, and the where when and how that they interact WITH your body- both inside AND out- is afundamental basis of taking charge of your health.
This post was co-authored by Jessie Johnson-Cash and based on her presentation at the USC Midwifery Education Day.
The human microbiome is rather fashionable in the world of science at the moment. The NIH Human Microbiome Project has
been set up to explore correlations between the microbiome and human
health and disease. To date the human microbiome as been associated
with, amongst other things obesity, cancer, mental health disorders,
asthma, and autism. In this post I am not going to provide a
comprehensive literature review – this has already been done, and the
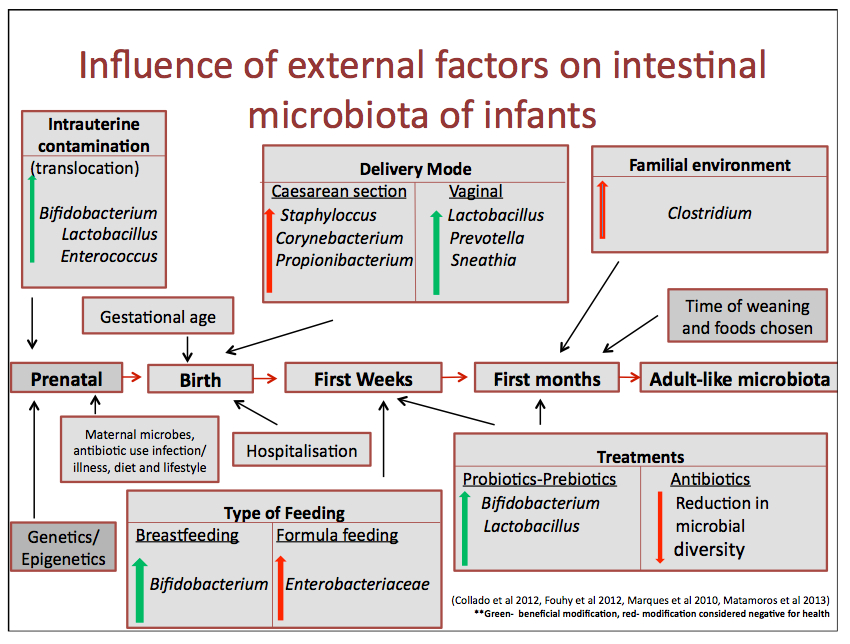
key reviews underpinning this discussion are: Matamoros et al. (2012) ‘development of intestinal microbiota in infants and its impact on health’and Collado et al. (2012)
‘microbial ecology and host-microbiota interactions during early life
stages’. Instead I am going to focus on what this means for pregnancy,
birth, mothering and midwifery. What is the human microbiome?
Based on a chart by Matamoro et al. 2013. Adapted and extended by Jessie Johnson-Cash.
Considerations for mothers and midwives
The following are not research based recommendations – the research
is yet to be done. They are more considerations/questions arising from
the developing knowledge around the human microbiome. There are quite a
few health practitioners writing about gut health currently – one of my
favourites is Chris Kresser because he includes references if you want to read the source of his information. Pre-conception and Pregnancy
The commonly accepted belief that the the baby inside the uterus is
sterile (whilst membranes are intact) is now being challenged. It seems
that maternal gut microbiota may be able to translocate to the
baby/placenta via the blood stream (Jiménez et al. 2008; Metamoros et al. 2013; Prince et al. 2014; Rautava et al. 2013; Zimmer 2013). Women’s gut microbiota change during pregnancy and this impacts on metabolism (Koren et al. 2012; Prince et al. 2014).
So ideally women need to head into pregnancy with a healthy microbiome
and then maintain it. Unfortunately our modern lifestyle is not very
microbiome friendly, and many of us have dysbiosis (an imbalance in gut
bacteria). Dysbiosis and too much of the ‘wrong’ bacteria has been
linked to premature rupture of membranes and premature birth (Fortner et al. 2014; Mysorekar & Cao 2014; Prince et al. 2014).
Suggestions:
You are what you eat… and you are the microbiota that you feed. Eat foods that nurture your microbiome: don’t eat toxins; eat fermentable fibres – starchy vegetables such as sweet potatos – they are microbiota food; eat fermented foods – kefir, sauerkraut etc. – they provide probiotics. Dietary probiotic foods may also assist with balancing vaginal microbiota (Hantoushzadeh et al. 2012; Rautava et al. 2013).
If your gut is damaged heal it and restore the balance of microbiota. This may involve taking probiotics.
Avoid antimicrobial skin products (eg. handwashes), and house cleaning products – you can watch a youtube explaining the FDAs concerns about such products.
"Dump the Jerk"..... I have said these very same words so many times to so many women. And I'm not talking about their husbands, boyfriends or significant others. I'm talking about their doctors.
This article rings so true for so many women in so many situations in so many places, but rings clearest for pregnant women and their choice (or lack thereof) care givers for their births. Sarah writes about one woman's experience with her Obstetrician:
"I recently heard through the grapevine about a woman whose doctor had scheduled a c-section because of suspected big baby. (She is of course weeks from her due date.) But, when the doctors vacation plans changed he no longer needed to schedule the c-section, and told her as much..."
I have heard several versions of this type of story myself, and each time my response was the same:
"Get the Hell out of there!!"
Women feel especially trapped once they get to 30 odd weeks and the true colours of their doctor start to show. They feel like it's impossible to change now. Where will they go? Who will take them on? What if they don't find someone else? They have a right to be concerned, even frightened, about changing everything at the last minute, but nothing is as scary as a doctor who's punching a time clock and pushing every woman through the same mold.
I have encourage several women to change their care provided in the last few weeks of their pregnancies, and worked with them to help them find another Doctor- or even better, a midwife!! It is possible. Many of the midwives I know will take on a client in this kind of situation no matter how close to their due date, regardless of how busy or "booked" they are.
But you'll never know if you don't ask! ;>P
Read this article- and pass it on to every woman you know that's stuck in this situation. Let them know that change is GOOD!!!
Dump The Jerk: Changing Care Providers Before it's too Late!!
The Jerk
So- your friends have introduced you to this "great"guy. He makes great money, has a nice car, big new house, good looking, all that seems important. You get a little closer a little faster than you would have liked and now you feel stuck in the relationship. As you get to know him better there are some things that really bother you about him.
You don't feel like he respects you at all. Whenever you mention something that is important to you he just blows it off. You have been wanting to go see a ballet for months and he just won't go- even though you go with him to countless monster truck shows. All of your opinions he would just rather not hear, and if you voice them anyways he makes a rude comment about how you don't really know anything. Sometimes he even scares you a little bit.
But- he is a great guy on paper, and all your friends love him. You have been going together for a few months now and it just feels like it would be too hard at this point to get out of the relationship. You hate being rude and hurting somebody's feelings anyway.
Of course you have a crazy, opinionated friend. She thinks a man should be respectful of you and what is important to you. Her husband treats her well, but doesn't have all that fancy stuff. She is actually happy in her relationship, unlike your friends. She keeps telling you to dump the jerk before it is too late, and you are stuck with him forever.
Seriously!
When we think about the above situation, it seems obvious right? Get out- find somebody good that you actually like and who likes you and respects you.
How many times do we hear this same stupid excuse though about somebody's doctor? "Oh, I am already 35 weeks, it is just too late to change." Or maybe this one, "Well, my sister went to this doctor too and I didn't know who else to go with. He is all right, and he tells me not to worry about anything."
It is not too late to change doctors until the cord has been cut. Am I being clear enough? We are talking about the birth of your baby. This is one of life's BIG events. It will change you. I am going to say that again, because it is so important. Birth will change you. How do you want your birth to change you? Do you want it to be full of regrets? Do you want to feel like a passive participant on a crazy ride where somebody else is behind the steering wheel? Or do you want your birth to be beautiful and empowering, like you hear it can be?
This is an Excellent Blog by Aruban Breastfeeding Mamas. Wendy talks about the need to speak the language to be able to communicate- in every situation in life this is true, but in childbirth it is VITALLY true!!
Beyond childbirth Wendy mentions breastfeeding as well, and this is such an important topic for new mothers. It seems that most new mothers think that breastfeeding will just happen, it's natural, right?!? Oh many will read a book or two, or at least a chapter or three in one of their pregnancy and birth books (if they read anything at all) on the subject of Breastfeeding, but rarely will they go any farther to prepare them selves for the journey than that.
My number one advice to all new moms-to-be is: Join a breastfeeding support group BEFORE baby arrives!! Be it a local informal group of breastfeeding moms who get together every few weeks for support and companionship, or a proper LLL meeting group. Which ever you're more comfortable with. Meeting with and seeing and talking with breastfeeding mothers while you're pregnant can make a huge difference when your own boobie baby arrives. If you've already met a few moms and have built even a tiny bit of a rapport with them, it will make it easier to be able to call on them for help should you need it. Learn the language of breastfeeding. It is vital to know and understand the language of the boob when your hungry babe wants to talk!!! If you can't find a group to teach you the language, then read a book. If you can learn even a few simple phrases in this language, you'll at least have enough of a handle on it to know HOW to ask for help and where to go to get help if you need it!!
The same with child birth. If you don't even know the simplest of phrases, how can you expect to be able to navigate your way through the insanity that medicalized birth can be?
The Language of Birth
You’ve been planning your vacation for many many months. After a lot of consideration you choose a country in which a foreign language is spoken. You’ve invested time in thinking where you want to go, and you’ve spent even longer saving up your money.
The day arrives and you’ve arrived at your long awaited destination. You made sure you had your bag packed well in advance. You have your clothes, something to read, possibly even music to relax you. As you get around this foreign country, slowly but surely you realize you’re in deep trouble… You know nothing of the language. The people speak to you, but you understand absolutely nothing. They tell you they’re taking you to a hotel of their choice, but you are starving and just want to eat, besides, you don’t even want to go to that hotel! But you’re practically helpless, no tolk, much less a dictionary. You figure, ‘ah, I’ll let them take me where they say is good, besides, they are the locals’. In the end, the vacation you’ve planned, and toiled for, all that you’ve envisioned that would relax you, is lost in the frustration of not planning well enough for the language barrier. You get back home, and you say to yourself ‘well….at least I am healthy and alive’
How many women, go through their pregnancies and births, and experience this situation? They painstakingly look for the right name for their child, they do their utmost to get the perfect furniture and the perfect color to match in the nursery. They expend almost all their money and time into the superficial matters of bringing a child into their lives, not anticipating the lasting effects of one of the most important days in their lives that is fast approaching, for which they feel ‘very prepared’ and yet very frightened. Family and friends ask if she’s got her stuff packed and ready. She says yes, she’s got her blankets, robes, socks, a novel to read and not to forget her toiletries. ‘I’ve got it all covered’, she figures.
She never looks up Childbirth Education classes, nor breastfeeding support groups and doesn’t even buy any pregnancy books. She does however look at televised birth stories on tv and learns a lot from them. She learns to fear pain and childbirth that is.
Surely enough, 38/2 weeks rolls around. Her doctor is pressing for induction because her ‘baby is huge, and her hips are simply too petite, besides..your baby is already full term!’ The doctor says she’d be fortunate enough if she could even have the baby vaginally. She shows up at the hospital for her induction, nervous but very excited that the baby will finally be here. She’s not sure what an induction actually is, but she’s put her full trust in her doctor “So what can go wrong?”.
Yet another new Blog that I've just discovered- "Don't get me Started" Rips into birthing in our society with an openness that is refreshing and shocking... But just as true, word for word.
Nine months along she comes waddling into the lobby. Checks in at the front desk, waits for a nurse escort. Yes her water has broken. Contractions are still far apart, no need to panic. It’s her first baby and she’s nervous. Scared of the pain. Doesn’t know how long this will take. In complete disbelief that she’s going to leave this hospital with a little being in her arms. Terrified of the unknown.
She’s dreamt of this day for nine months. Read all the books about what to ‘expect’ and yet there was no chapter on giving up rights. There was no chapter on becoming powerless.
Once her water breaks, she can’t leave her bed. Once we give you pitocin or an epidural, don’t even think about moving. Psychiatric patients are never put in restraints, never tied down (except for the worst of the worst situations) because it is “cruel and unusual punishment”. But laboring women? Laboring women are put in medical restraints. Pharmacologic restraints. We pump medicine through an IV, shove it into the space in your spine and say DON’T MOVE. YOU CANNOT MOVE. DON’T EVEN THINK ABOUT FUCKING MOVING.
We don’t care that you hurt. We don’t care that it’s better and safer for the baby and for you to move, move, move. You can’t move. It’s hospital “policy”. “Policy” that was created for the convenience of clinical staff. There is zero evidence saying this is a good idea. In fact, the evidence states quite the contrary. To move, move, move. To shift positions and let gravity help you. To take a walk and have a massage and lay in a bathtub. Actual scientific evidence tells us that this is what women SHOULD be doing. Instead, the medical establishment drips an IV, pushes the meds and takes choice away from women. Every second of every minute of every hour in this country a woman’s choice is being ripped from her.
She lays in pain. Vaguely remembering what she wanted to happen. How she dreamt this day was going to go. She read the books, rented the videos; hell, she read the blogs and watched the YouTubes. There are so many options out there! So many choices! Look at all these different ways I can maneuever my own body to get this baby out of here. Nope.
None of those things happened. Wait. Where are those choices now?
Now she’s medicated against her will. Now she’s lying in a clouded haze. Never told the side effects. Has no idea those meds will depress her breathing, her heart rate, her level of consciousness. Maybe they mentioned the drugs can “cross the placenta” but she was also conveniently told in a moment of horrific vulnerability that the meds will “take her pain away”.
And after a quick nap, it’s been decided. While she was out cold, and the baby’s heart rate slowed and that little swimming baby in the happy amniotic fluid struggles to keep it together, it’s decided. She hasn’t progressed. Not dilated far enough. Not effaced. Sure the meds caused this. Sure the meds we pumped in to her to “stop the pain” pulled the e-break on her labor. The very meds we gave her, we insisted that she take, stopped the body from doing the very natural thing that we’ve been doing for millions of years. The solution? Cut her open! Yay for sugery!
“You haven’t progressed enough. We’re going to have to do surgery.”
That is not choice. That is a directive. That is an order. That is not garnering consent. That is not providing all the options. That is not laying out the risks for surgery and the risks against surgery. It’s a fucking chop shop in there.
We call them “pre-dinner Cs” for a reason. Lord knows that obstetrician wants to get home for dinner so it’s no surprise that she’s induced at 2ish and delivers via c-section by 3ish. Knocked out in another drug-induced haze. Baby ripped out of her belly, placed in a plastic bin like a bag of lettuce at Safeway. Lay her on the mother’s chest? Heaven forbid the baby’s “yucky”. Heaven forbid the baby start breasfeeding, doing that other thing we’ve been doing for millions of years.
Nope. The doctor and nurses have exams to do. They need to poke and prod and shove under a light. Heaven forbid they learn to do an assessment while the baby is in it’s most natural position, with mom.
~~~~~~~~~~~~
Every day I walk in to clinical my heart races. I clinch my fists, grind my teeth. Nothing about this experience is what it is supposed to be like. I have never had a being growing inside of me. I’ve never felt a kick or a flutter or a summersault inside of me. I have never expected and waited and read and dreamt of this day. And yet. There I go and stand in disbelief.
And watch from behind a wall of horror as these women are objectified and victimized. There are no options, no choice, no bevy of laboring menu items in which to check off. Fuck, there are more options at a Taco Bell drive-thru than there are in your average laboring suite in an American hospital.
I make no jugements about your own delivery. If you wanted to be drugged and not “feel anything” (*ahem* a ridiculous expectation that the medical establishment shoves into women’s psyhe) or scheduled your own c-section, that’s lovely. Hats off to you. I am not pointing fingers at you and saying we all need to do it the same.
This is about choice.
At our most vulnerable moment. When we are terrified and filled with hormones and emotions and doubt and stabbing, murderous pain. We will do anything.
You know what I would do? You know what I plan to do? I will risk it all and birth on my kitchen floor before I allow any fucking person in scrubs to come near me and take away my choice. To tell me “what is best for the baby” when I know damn well they’re lying. Fucking lying. Lying cause they’re impatient. Lying cause drugs have a higher reimbursement rate. Lying because they want control over my body and this process. I will push out a baby (if I am blessed with that option), in a bathtub, in a manger lined with hay before I trust a sole in the laboring unit in any American hospital.
Musings of a Montreal Doula has written yet another very insightful blog : "honouring a woman's intuition"
To me, this is yet another prime example of the medical machine's invisible interventions (Which I am currently writing an article on). A woman in pregnancy and in childbirth is at her peak of feminine power, and more in tune with her body than ever before. When she is supported and honoured, she is allowed to hear her body and to act in freedom as she needs to: to grow her beautiful healthy baby and to give birth in a calm and secure environment.
As I posted a couple of days ago, the US Dept of Defence has put together a great "Emergency Childbirth Guide" with the basic premise being "Just leave well enough alone and let the birthing mother get on with it!!" Yet medical professionals in L&D wards across North America seem to be incapable of this- to the point that they will ignore a birthing woman's intuition completely and stick with their own agenda. To me this is one of the most insidious of the invisible medical interventions that overpowers pregnant and birthing women. It is bad enough that most women are forced to conform to the hospital and doctors rules & regulations and are forced through a one size fits all cookie cutter birthing factory, but when even your own voice is taken from you, you are literally stripped down to just another number.
Like Musings of a Montreal Doula, I have listened to so many stories of women who have had very powerful insights into their labours and pregnancies, yet unfortunately most of these have been ignored. Women who've KNOWN that something has been wrong during their labour only to be shushed and treated as a naughty child who's carrying on too much.... only to give birth to a very sick baby that has to spend weeks in NICU.... because no one would listen. Women who've shown up at L&D because they've KNOWN that they are in serious labour, to have medical staff laugh at them and try to send them away "Sweetheart, if you were really in labour right now, you'd know about it!!"... only to give birth 15 minutes later into the startled ungloved hands of a shocked maternity ward nurse.
In pregnancy I see it all the time with so called "Due Dates". A woman has a positive pregnancy test and is sent for an Ultra Sound to date the pregnancy where some Technician Tells the woman when she will have her baby. I can not count the amount of times I've heard women say 'That can't be right"... "I'm at least 2 weeks farther along/not that far along"... and yet even though it is their own body that they are growing these babies in- bodies they've lived with their whole lives.... the doctors invariably go with the U/S pictures "Due Date". This happened to me during my pregnancy with my second daughter. The Ultra Sound technicial grandly announced a due date that I KNEW was at least 2.5-3 weeks earlier than I expected..... hell, not "expected" I KNEW exactly when I had ovulated, and exactly how far along I was. But as usual the doctor chose to believe the pictures. So my daughter was born at "40wks3 days".... weighing 5 lb 15 oz. I gave the doctor a look that said "I told you so", and he just shrugged. A good friend of mine was assigned a due date with her youngest child that was 3 weeks later than she knew her actual due date was. She told her doctor several times that "this baby needs to come out now"... only to be patted on the head like a small child and told "Oh, every woman gets tired of being pregnant at this stage...." When she went into labour on her "due date" everyone in the birthing room again Pooh poohed her severe anxiety over the health of her baby through a traumatically fast and powerful birth... only to be shocked when her very obviously past term baby was born having convulsions from laying in a stew of miconium thicker than tar. If doctors had listened to her intuition, her baby might not of spent a week in NICU on respirators.
Intuition is a powerful tool, and an empowering tool for women to listen too. Only by listening to our selves and our inner voice and our body can we truly be liberated and empowered to make the decisions that we KNOW are best for us and our babies.
One of the sad things about today's care of the pregnant/birthing/postpartum woman is a lack of respect for her intuition. Many women are considered hysterical or completely blown off for discussing their intuitions. What exactly is intuition? It's about looking inside and gathering information about things and situations not by reason, but by feeling. It is not about being psychic. When we refer to intuition, people sometimes think we're refering to looking into the future, which, unless you truly are gifted with psychic ability, is not generally possible. I think intuition just means gathering information about things which are conveyed in ways more subtle than can be perceived by the five senses. I don't believe, as doulas, we can predict how birth will ultimately play out in the future (try to pin Birth down, and she changes on you...she hates us puny humans trying to "know" her too well), but you can, in the here and now, be able to intuit something about a woman, perhaps an emotional or energetic frequency, that can give you a good or not so good feeling about how that may play out in the field of childbirth. And you can be wrong, which is okay, because nothing is fool proof.. not ultrasounds, amnios, or blood tests (oh my!). ...
...I trust women. A woman in her childbearing year tends to have incredible insight into the workings of her body and her baby. She should be given plenty of space to talk about these feelings freely without fear of being judged as "silly". When you're growing a baby inside you, you are linked to another being more intimately than any other way. It is no surprise that a woman can have very strong feelings about what's going on with her baby. I kinda believe that a baby transmits his feelings to his mom in some cases. I don't think he says, "Mother, I am planning on becoming photographer someday," or "Ma, I will be born with a large birthmark." In fact, many women before the days of ultrasound were unaware they were carrying twins until the day of their birth. I just mean I have seen wild flashes of insight which, in spite of medical disbelief or logic, have been proven right. There are just times a woman tells you something when you know in your own gut what she is saying is incontrovertible...you know it by a strong feeling of resonance with the truth of her words.
Here are a few examples. A really crazy amazing wild woman friend of mine named Michelle, was my doula for the birth of my first child. She had given birth to her own first three children at home in the mountains of Tennessee, one of them unassisted, I believe. When she became pregnant with her fourth child, she had been doing some doula work in hospitals. She told me she thought she'd birth this baby in a hospital. I asked her, "What do you mean? You've had great home births. What makes you want to go to the hospital?" She told me she wasn't sure, just that she had felt really comfortable in a certain hospital she had worked at, and felt drawn to give birth there. She arrived at the hospital in labour, and was very quickly rushed to the OR for an emergency C-section because of severe fetal distress due a real and serious umbilical cord problem. Her son was fine. And her next three children were born at home in the Dominican Republic.
This has come up quite a bit lately. I always seem to come across someone who touts the old line of "I was/did/had _____ and turned out just fine. My child will too." You can fill this in with "I was formula fed, and turned out just fine.", or "I was delivered by cesarean, and turned out just fine.", or any of the other things that are PROVEN to be less healthy for babies. Why do people justify less healthy choices with completely anecdotal ( and often incorrect ) evidence? Unfortunately, it's much easier to continue with this mindset, than to admit that you could have done better for your child(ren), or yourself.
“We hold these truths to be self-evident, that all men [and women] are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.”(US Declaration of Independence)
Every mother and baby has the right to be treated with reverence and respect during the birth process, including pregnancy and beyond.
When a woman becomes pregnant, she and her baby have unalienable rights. First, the right to life: In June of this year, the United Nations Human Rights Council adopted a landmark resolution acknowledging maternal mortality and morbidity as a human rights issue.(1) The adoption of this resolution prods governments to “change the way they view maternal death—that is, as a human rights issue no less serious than executions, arbitrary detentions, or torture.”(2)
Next, the right to liberty: The word “liberty” contains aspects of freedom, independence, autonomy, emancipation. These concepts are not usually considered in relation to the childbearing year. It is time to declare that mothers and babies have the right to liberty in pregnancy and birth.
Finally, the pursuit of happiness is of utmost importance to those of us who care for mothers and babies. Most births around the world lead to some varying degree of preventable trauma for the mother and baby. I say it is preventable because much of it is iatrogenic, caused by the doctor or midwife. In many cases, if the mother, baby and birthing process had been treated with respect, the trauma would possibly have never taken place. Instead, the mother likely would have had the most miraculous experience of her life. At the very least, she would have felt a part of the decision-making process if things still did not go as planned. Birth today is a doctor dictatorship in many practices and in many hospitals. Mothers and babies are missing the healthiest possible beginning, both physically and emotionally. Their human rights are being violated.
Pregnancy and birth are usually the most crucial and powerful passages in a woman’s life. This can be perceived by the mother as either a powerfully great experience or a traumatic ordeal. Mom will generally have one of these reactions and those feelings will last her entire life, even if they are buried in the busy job of mothering. She will either soar at the thought of her birth or be driven to the depths of sorrow, especially in this age of the cesarean cut. The same is true of the way the birth experience imprints on the baby. Though he or she may not consciously remember it, the experience will have many life-long effects on the child.
Having posted that horrifying video this morning of an over sized barbie giving birth..... *shudder*.... I've been thinking on the topic of how medicalize birth has endangered women and babies. and thinking about the horrible truth: that it has become so mainstream, so "Normal", so Accepted, that women and their partners don't even question it any more.
Not a week, not a day goes by that I don't read comments on birthing/pregnancy forums about scheduled inductions and caesarean sections or about women planning their epidurals in advance. Birth stories of women told the most outrageous lies by the medical machine to validate the doctors opinion of why all these interventions are necessary.
I have days when I literally rant at the computer screen (these days apparently happen often enough that my kids no longer even take note, lol), and I want to scream, to tell these women that NO! They don't need to labour on their backs strapped to a plethora of monitors, with an IV and epidural in place. ...... ARGH!!!!
I tell people and try to educate people all the time- both in real life and online- I try to make people aware that THEY need to do the research and find out for themselves. And I post articles and studies to try to open the eyes of those that are blinded by faith in a medical machine that plays to a different drum.
This is one of my most favorite articles ever written on the topic of Birth and the dangers and risks of interventions. I have lost count of how many times I've posted this article on Forums, blogs, chats, web sites, Facebook...... If every pregnant woman and her partner read this article, I'm SURE that at least some of them would wake up from their stupor and see the reality of modern child birth.
A woman in Iowa was recently referred to a university hospital during her labor because of possible complications. There, it was decided that a cesarean section should be done. After the surgery was completed and the woman was resting post-operatively in her hospital room, she went into shock and died. An autopsy showed that during the cesarean section the surgeon had accidentally nicked the woman's aorta, the biggest artery in the body, leading to internal hemorrhage, shock and death.
Cesarean section can save the life of the mother or her baby. Cesarean section can also kill a mother or her baby. How can this be? Because every single procedure or technology used during pregnancy and birth carries risks, both for mother and baby. The decision to use technology is a judgment call—it may make things either better or worse.
We are living in the age of technology. Ever since we succeeded in going to the moon, we have believed that technology can do everything to solve all of our problems. So it should come as no surprise that doctors and hospitals are using more and more technology on pregnant and birthing women. Has it solved all the problems that can arise during birth? Hardly. Let's look at the recent track record.
Has the recent increasing use of technology during pregnancy and birth resulted in fewer damaged or dead babies? In the United States there has been no decrease in the past 30 years in the number of babies with cerebral palsy. The biggest killer of newborn babies is a birth weight that is too low, but the number of too-small babies born has not decreased the past 20 years. The number of babies who die while still in the womb has not decreased in more than a decade. While the past 10 years has seen a slight drop in the number of babies who die during their first week after birth, the scientific data suggest an increase in the number of babies who survive the first week but have permanent brain damage.
Is the increasing use of technology saving the lives of more pregnant and birthing women? In the United States the scientific data show no decrease during the past 10 years in the number of women who die around the time of birth (maternal mortality). In fact, recent data suggest a frightening increase in the number of women dying during pregnancy and birth in the United States. So it may be that the increase in the use of birth technologies is not only not saving more women's lives but it is also killing more women. This possibility has a reasonable scientific explanation: cesarean section and epidural anesthesia have both been used more and more in this country and we know that both cesarean section and epidural block can result in death....